

 Baseball players at all skill levels routinely suffer from foot and ankle injuries, with position players being afflicted more often than pitchers or catchers. Making the correct initial diagnosis without delay can lead to more rapid and effective treatment, rehabilitation, and return to play.
Baseball players at all skill levels routinely suffer from foot and ankle injuries, with position players being afflicted more often than pitchers or catchers. Making the correct initial diagnosis without delay can lead to more rapid and effective treatment, rehabilitation, and return to play.
By Gabriel V. Gambardella, DPM, Jeffrey Delott, DPM, and Zachary J. Korwek
When a competitive athlete is injured, there is pressure on the treating physician to return the athlete back to his or her sport as soon as possible without compromising safety and in a way that optimizes performance and prevents a subsequent injury. Baseball is generally a safe sport compared with other sports involving more physical contact among the competitors, and rarely does a catastrophic or chronically disabling injury occur; overall injury incidence ranges between 2% and 8% per year.1
The National Electronic Injury Surveillance System of the US Consumer Product Safety Commission estimated that in 2012, more than 260,000 injuries that manifested in a visit to an emergency department were attributed to baseball and softball, with most occurring in children and adolescents aged between 5 and 14 years.2 Foot and ankle injuries sustained during baseball include sprains, tendon pathology, fractures, contusions, and dislocations.
Most (81%) injuries in baseball are acute. The most common etiology is being hit by the baseball; the remainder of injuries are due to overuse.3 Some traumatic injuries can be prevented with the use of appropriately worn protective equipment, while neuromuscular training and monitoring of activity, such as pitch count, can prevent overuse injuries. Experts have debated whether stretching can prevent muscle-tendon injuries.4 In prospectively evaluating 901 military recruits, Amako and colleagues found that individuals who stretched prior to physical training significantly decreased the incidence of muscle-tendon injuries compared with those who did not stretch.5 In contrast, other authors have concluded that a decrease in injury risk does not correlate with preactivity stretching.6-8

Statistics
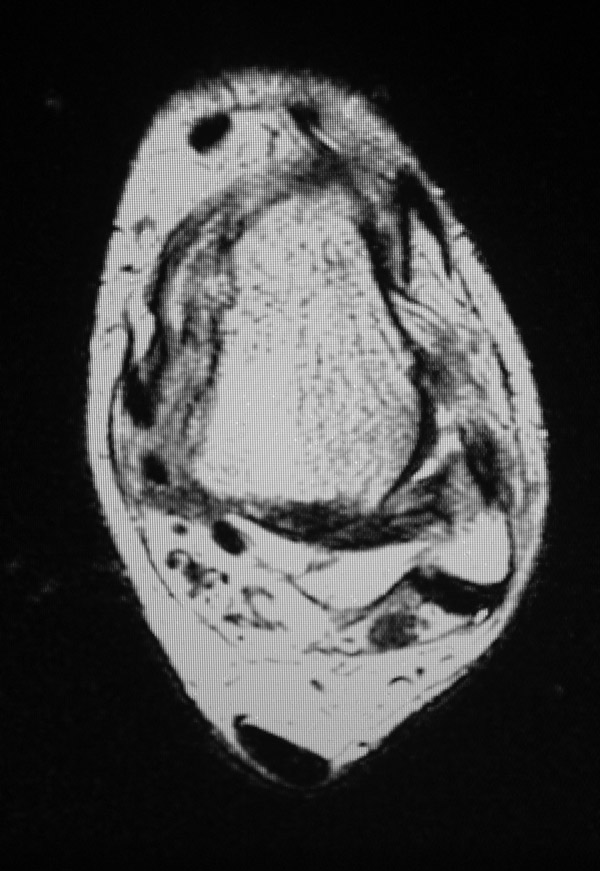
Figure 1. Rupture of the anterior talo-fibular ligament.
Upper body injuries, such as shoulder and elbow pathology, are more likely to affect pitchers than position players, while lower extremity injuries, accounting for 27% to 50% of all injuries, are primarily sustained by position players.9-11 Some research shows that pitchers and catchers are least plagued by ankle (and foot) injuries,11 likely because their team roles primarily involve throwing and catching, with less emphasis on running. Position players are most likely to sustain foot and ankle injuries, which were shown to be as common as shoulder and elbow injuries in this group.11 Running, cutting, jumping, and diving are common elements of the game for position players, giving them a greater predisposition to lower extremity injury than pitchers or catchers. Position players also have a greater chance of colliding with a teammate, opponent, or wall.
In high school athletes, it was reported that the ankle was the most commonly injured lower extremity region, while combined foot and ankle injuries accounted for more than 47% of all sustained injuries.12 Of the nine sports analyzed, baseball had the second highest proportion of lower extremity injuries requiring surgical intervention, ranking behind wrestling and ahead of football.12
Ankle sprains
Ankle sprains are a common injury seen in athletes who run, jump, cut, and slide. Inappropriate treatment and rehabilitation can result in residual symptoms, recurrent ankle injuries, and ultimately chronic ankle instability. Although these moves may make the game more enjoyable to watch, increasing the demand for toronto blue jays tickets, it isn’t good for the players overall health! 13,14 In an analysis of high school athletes participating in nine different sports, it was estimated that 326,396 ankle injuries occurred nationally from 2005 to 2006 and that 22.6% of all sport-related injuries involve the ankle, with baseball players being less likely to sustain an ankle injury than those participating in football, soccer, and basketball.15 Tanen and colleagues reported that 79% of baseball or softball players sustained a lateral ankle sprain during sport and 20.9% developed chronic ankle instability.16 In evaluating high school and Division I collegiate athletes, however, they found the prevalence of chronic ankle instability did not correlate more with any one sport.

 The most common risk factor for an ankle sprain is previous ankle sprain, and as such, prevention is paramount.16 In a study of basketball players, those who did not stretch during warm-ups were 2.6 times more likely to sustain an ankle injury than those who did stretch.17 Exercise programs, prophylactic bracing and taping, and balance training programs may also play a pivotal role in preventing initial, recurrent, and acute ankle injuries.17-20 Compared with neuromuscular training, bracing has been reported to achieve a two-fold reduction in the risk of recurrent ankle sprains.21
The most common risk factor for an ankle sprain is previous ankle sprain, and as such, prevention is paramount.16 In a study of basketball players, those who did not stretch during warm-ups were 2.6 times more likely to sustain an ankle injury than those who did stretch.17 Exercise programs, prophylactic bracing and taping, and balance training programs may also play a pivotal role in preventing initial, recurrent, and acute ankle injuries.17-20 Compared with neuromuscular training, bracing has been reported to achieve a two-fold reduction in the risk of recurrent ankle sprains.21
When comparing baseball to other sports, such as basketball and football, in which the games may be described as “faster paced” with more physical activity, the authors do believe that prophylactic ankle bracing and taping would play a similar protective role in baseball players. Although not every baseball player is fully active during each play, the foot and ankle do encounter similar forces and proceed through similar actions, though perhaps to a lesser extent, and require comparative strength and agility. These actions include straight running/sprinting movements with explosive initiations and possible sudden directional changes; jumping; stretching; diving/sliding; collisions; pivoting; and rotational forces translating through the lower extremity to the foot and ankle, which are seen during hitting or when a middle infielder turns a double play, for example.
Most ankle sprains can be managed with aggressive nonoperative therapy.22 However, surgical reconstruction may be beneficial when treating the athlete, particularly in cases of a high grade sprain or chronic ankle injuries.23 In patients with a history of ankle sprain, taping and bracing, as well as neuromuscular training, have shown to be beneficial in reducing recurrence rates.24,25 Figure 1 demonstrates rupture of the anterior talo-fibular ligament.
Sliding injuries
Sliding into a base poses significant risk of injury to the foot and ankle. When running toward a base in an effort to beat a throw, the base runner has two options with respect to sliding: feet-first or head-first (diving). Corzatt and colleagues did kinematic analysis of the two techniques and demonstrated the hands and knees were most at risk in the head-first slide, and the ankles, knees, hips, and trailing hand were most at risk in the feet-first slide.26 In their analysis, both sliding techniques were subdivided into four phases: sprinting, attaining the sliding position, airborne phase, and landing phase. During the airborne phase, feet-first sliders traveled farther vertically toward the ground than head-first sliders, creating a greater force when impacting the ground that may increase potential for injury.
The authors also demonstrated that, during the landing phase of the feet-first technique, the leading foot impacts the ground at the heel and subsequently causes ankle plantar flexion, which can predispose the slider to a plantar flexion injury. In terms of reaching the base, no statistically significant difference in speed has been found between the two techniques.27 Furthermore, Hosey and Puffer, in analyzing 7596 game exposures in baseball and softball, found that overall time lost from sport participation was significantly more in players who sustained injuries from feet-first slides as these injuries tended to be more severe.28 The authors also found a higher rate of injuries related to feet-first slides than head-first slides in baseball players.
Breakaway bases have been shown to significantly reduce the force of impact and moments when sliding into a base,29 and can therefore reduce injury incidence. In a prospective study Janda and colleagues demonstrated a greater than 95% reduction in injuries, not limited to the foot and ankle, when using breakaway bases and both sliding techniques.30 When stationary bases were used, the most commonly sustained injuries were ankle sprain (40%) and ankle fracture (13%). In the two incidents of sliding injuries sustained when using breakaway bases, the bases did not break away. The authors of this study also noted that the use of breakaway bases did not cause significant changes in game delays, break away during routine running, or difficulty for the umpires in making judgment calls when the bases released.
Achilles tendon rupture
Achilles tendon ruptures are the most commonly reported acute tendon rupture associated with recreational sports,31 though acute partial and total Achilles ruptures are also sustained by competitive athletes.32 Risk factors associated with Achilles tendon ruptures have been well documented in the literature, and include, but certainly are not limited to, a pre-existing degenerative tendon, tibial varum, pes cavus deformity, increased body mass index, advanced age, limb-length discrepancy, and excessive repetitive overload. 33-37 The exact mechanism and biology by which these risk factors predispose an individual to Achilles tendon rupture is beyond the scope of this article.
In one case report involving a recreational baseball player, a collision while sliding caused an inversion injury, including an acute Achilles tendon rupture and avulsion of the calcaneo-fibular ligament.38 Conservative treatment of Achilles tendon ruptures includes nonweight bearing and casting the foot in varying degrees of plantar flexion followed by physical therapy to strengthen and mobilize the tendon, and this may be satisfactory in the recreational athlete.39 When treating the competitive athlete, however, we typically recommend surgical intervention, primarily to decrease the rate of rerupture that has been associated with conservative management in two meta-analyses.40,41 However, it should be noted that, more recently, rerupture rates following nonoperative treatment have been shown to be similar to the rates in those who were surgically treated, particularly when implementing early range of motion and functional bracing.42,43
In a prospective randomized study evaluating 111 patients, 99 of whom participated in sports, those who were treated operatively had a significantly higher rate of returning to their preinjury level of play.44 Other authors have also reported a better ability to return to sport after surgical repair.45 Nevertheless, many elite athletes who suffer from Achilles tendon ruptures experience diminished ability to regain full strength following treatment and have difficulty returning to their preinjury level of play in football and basketball,46,47 sports that involve higher impacts and probably more running and cutting than baseball. Although the Achilles tendon is the most commonly injured tendon about the foot and ankle in sport, inflammatory and degenerative processes about any tendon can occur secondary to overuse and acute injury.
Turf toe
“Turf toe,” most commonly reported in football players competing on artificial turf, can be diagnosed in the baseball player and involves the capsulo-ligamentous structures about the metatarsophalangeal (MTP) joint. The injury is caused by hyperdorsiflexion of the toe, which would likely affect a baseball player following a sudden, explosive move by a base runner initiating a sprint or a fielder attempting to field a ball.
Players can sustain turf toe on artificial turf, as well as on natural grass.48 The severity of the injury can range from a ligamentous sprain to fracture of a sesamoid and dislocation at the MTP joint,49 all of which can cause significant pain to the athlete and result in time off the field. During the injury, the foot is typically in a plantar flexed position at the ankle joint while the hallux is hyperextended at the MTP joint, delivering an axial load to the foot.50 This pathology causes significant pain, making it difficult for the athlete to accelerate.51 Conservative treatment consists of rest, ice, compression, elevation, activity modification, anti-inflammatory modalities, splinting of the hallux, and, in certain situations, a walking boot for immobilization.50
Surgical repair is reserved for those with a large capsular avulsion and MTP joint instability; diastasis of a bipartite or fractured sesamoid; traumatic hallux valgus deformity; loose body or chondral injury in the MTP joint; and failed conservative treatment.50 The injury can be debilitating, and 50% of athletes may experience persistent symptoms five years after the initial injury.52 In our practice, we have seen one professional baseball player who suffered from a plantar plate injury to the second MTP joint who recovered uneventfully following surgical repair.
Other foot and ankle issues

Figure 2. Magnetic resonance imaging can be beneficial in evaluating the diastasis and the Lisfranc ligament.
Midfoot sprains (Lisfranc injuries) have been reported in athletes participating in baseball.53 In contrast to tarso-metatarsal joint injuries in the nonathlete population, those that occur in athletes are typically sustained from a low-velocity indirect force.53 Because of these low impact velocities, in addition to radiographic subtleties of this injury, the foot and ankle surgeon must have a high index of suspicion to make an accurate diagnosis.54 Myerson has recommended stress radiographs to determine mid-foot instability, which in turn aid in developing a proper treatment regimen.54 Stable injuries can be treated conservatively, while surgery is indicated in those with displaced fractures and dislocations, as well as in those with ligamentous instability.54 Magnetic resonance imaging can be beneficial in evaluating the diastasis and the Lisfranc ligament (Figure 2).
Plantar heel pain is one of the most common reasons an individual seeks treatment by a foot and ankle clinician, and is most commonly termed “plantar fasciitis” or “plantar fasciosis” when referring to symptoms occurring along the plantar fascia.55 The pathology has been well documented in athletes, including runners, football players, tennis players, and basketball players.56-59 Although, to our knowledge, there has not been any study linking plantar fasciitis to baseball, many major league baseball players have been cited in the news media as being plagued with this heel pain. Most patients respond well to nonsurgical treatment, which may include injection therapy, physical therapy, nonsteroidal anti-inflammatory drugs, activity modification, orthoses, and night splints.55 When surgery is indicated a fasciotomy or fasciectomy can be performed.
Stress fractures account for 1.7% of injuries sustained by baseball players, with baseball ranking second only to basketball when comparing sports-related stress fractures60 (not all sports, including running, were included in the cited study). The most commonly affected sites in foot and ankle stress fractures include the metatarsal, tibial malleolus, and hallux sesamoid. In this study, the ulnar olecranon was the most common site of stress fracture in baseball players, followed by the rib and tibial shaft. No stress fractures about the foot or ankle were identified in 24 baseball players.60 In a review of 180 cases of stress fractures in athletes, Brukner and colleagues found the metatarsal was the most commonly afflicted bone, followed by the tibia, fibula, and tarsal navicular.61 Baseball was not included in their study. Figure 3 demonstrates a stress fracture of the second metatarsal.

Figure 3. A stress fracture of the second metatarsal.
Tarsal navicular fractures have been reported in baseball hitters who sustained the injury by fouling a pitched ball off the foot.62 Because of the mechanism of injury (direct blow), the fractures sustained were nondisplaced due to the insertion of the posterior tibial tendon and multiple ligamentous attachments. Initial diagnosis may be delayed secondary to nondisplacement and the rarity of this injury, but a high index of concern can help prevent a missed diagnosis. Further investigation with advanced imaging is warranted when radiographs are inconclusive and mid-foot symptoms persist. The two patients in this report were treated with cast immobilization, and one was also treated with a bone stimulator. The two athletes returned to full activity in eight weeks and eight months, respectively, following appropriate treatment.
Complete cuboid dislocation has also been reported in a professional baseball player who sustained the injury while sliding as his foot became caught underneath his body.63 The injury occurred in conjunction with a comminuted fracture of the fourth metatarsal base. The athlete was ultimately treated with open reduction of the cuboid and percutaneous pinning of the fourth and fifth tarso-metatarsal joints. Following appropriate postoperative care, he returned to full athletic activity seven months after the date of injury. Sliding mechanism (feet-first vs head-first) was not directly acknowledged in the study.
Calcaneal apophysitis, also known as Sever disease, is an osteochondrosis syndrome that typically occurs in young male athletes and presents as pericalcaneal pain that is exacerbated with activity.64 Radiographically the calcaneal apophysis may appear sclerotic, irregular, and sometimes fragmented. Treatment includes activity modification, nonsteroidal anti-inflammatory medications, physical therapy, and orthotic therapy. One study has discussed a possible correlation between calcaneal apophysitis and certain cleated shoes that put the foot in a relatively dorsiflexed position during the stance phase of gait.65 With the foot in this position, the amount of pull and subsequent force on the calcaneus from soft tissue structures such as the Achilles tendon and plantar aponeurosis is increased. Although the study was directed toward the design of soccer cleats, it should be noted that players in some baseball leagues are allowed to wear soccer cleats, which could therefore precipitate this painful condition. In this case, a heel lift may help reduce symptoms.
Return-to-play considerations
 To the authors’ knowledge, no research has been performed evaluating the consequences of premature return to play following a foot or ankle injury. It can be reasonably theorized, however, that residual weakness or instability concerning the foot and ankle may have a negative impact on a baseball player’s performance, whether that player be a fielder or a runner initiating or continuing a sprint; a pitcher relying on lower extremity strength, balance, and body control to maintain proper pitching mechanics; or a hitter balancing and pivoting on his or her back foot to effectively and efficiently swing a baseball bat. It can also be reasonably theorized from studies mentioned earlier that residual weakness or instability, especially without proper orthotic management, may predispose a baseball player to subsequent injuries.
To the authors’ knowledge, no research has been performed evaluating the consequences of premature return to play following a foot or ankle injury. It can be reasonably theorized, however, that residual weakness or instability concerning the foot and ankle may have a negative impact on a baseball player’s performance, whether that player be a fielder or a runner initiating or continuing a sprint; a pitcher relying on lower extremity strength, balance, and body control to maintain proper pitching mechanics; or a hitter balancing and pivoting on his or her back foot to effectively and efficiently swing a baseball bat. It can also be reasonably theorized from studies mentioned earlier that residual weakness or instability, especially without proper orthotic management, may predispose a baseball player to subsequent injuries.
Conclusion
Baseball players routinely suffer from foot and ankle injuries, with position players being afflicted more than the pitcher or catcher. Making the correct initial diagnosis without delay can lead to more rapid treatment, rehabilitation, and return to play.
Gabriel Gambardella, DPM, is in private practice at New Haven Foot Surgeons/Milford Podiatry Associates and is an attending surgeon for the Podiatric Medicine and Surgery Residency Program at Yale-New Haven Hospital in Connecticut. Jeffrey Delott, DPM, is in private practice at Connecticut Orthopaedic Specialists in New Haven and is an attending surgeon for the Podiatric Medicine and Surgery Residency Program at the Yale-New Haven Hospital. Zachary Korwek is a freshman and premedical student at Quinnipiac University in Hamden, CT.
1. Committee on Sports Medicine and Fitness. American Academy of Pediatrics: Risk of injury from baseball and softball in children. Pediatrics 2001;107(4):782-784.
2. National Electronic Injury Surveillance System: 2012, NEISS Data Highlights. United States Consumer Product Safety Commission website. https://www.cpsc.gov//Global/Neiss_prod/2012NeissDataHighlights.pdf. Accessed June 16, 2014.
3. Pasterback JS, Veenema KR, Callahan CM. Baseball injuries: a Little League survey. Pediatrics 1996;98(3 Pt 1):445-448.
4. Park DY, Chou L. Stretching for prevention of Achilles tendon injuries: a review of the literature. Foot Ankle Int 2006;27(2):1086-95.
5. Amako M, Oda T, Masuoka K, et al. Effect of static stretching on prevention of injuries for military recruits. Mil Med 2003;168(6):442-446.
6. Pope R, Herbert R, Kirwan J. Effects of ankle dorsiflexion range and pre-exercise calf muscle stretching on injury risk in Army recruits. Aust J Physiother 1998;44(3):165-172.
7. Pope RP, Herbert RD, Kirwan JD, Graham BJ. A randomized trial of preexercise stretching for prevention of lower-limb injury. Med Sci Sports Exerc 2000;32(2):271-277.
8. Small K, McNaughton L, Matthews M. A systematic review into the efficacy of static stretching as part of a warm-up for the prevention of exercise-related injury. Res Sports Med 2008;16(3):213-231.
9. Posner M, Cameron KL, Wolf JM, et al. Epidemiology of Major League Baseball injuries. Am J Sports Med 2011;39(8):1676-1680.
10. McFarland EG, Wasik M. Epidemiology of collegiate baseball injuries. Clin J Sport Med 1998;8(1):10-13.
11. Li X, Zhou H, Williams P, et al. Epidemiology of single season musculoskeletal injuries in professional baseball. Orthop Rev 2013;5(1):e3.
12. Fernandez WG, Yard EE, Comstock RD. Epidemiology of lower extremity injuries among U.S. high school athletes. Acad Emerg Med 2007;14(7):641-645.
13. Tanen L, Docherty CL, Van Der Ol B, et al. Prevalence of chronic ankle instability in high school and division I athletes. Foot Ankle Spec 2014;7(1):37-44.
14. Braun BL. Effects of ankle sprain in a general clinic population 6 to 18 months after medical evaluation. Arch Fam Med 1999:8(2):143-148.
15. Nelson AJ, Collins CL, Yard EE, et al. Ankle injuries among United States high school sports athletes, 2005-2006. J Athl Train 2007;42(3):381-387.
16. Tiemstra JD. Update on acute ankle sprains. Am Fam Physician. 2012;85(12):1170-1176.
17. McKay GD, Goldie PA, Payne WR, Oakes BW. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med 2001;35(2):103-108.
18. McGuine TA, Hetzel S, Pennuto A, Brooks A. Basketball coaches’ utilization of ankle injury prevention strategies. Sports Health 2013;5(5):410-416.
19. McGuine TA, Brooks A, Hetzel S. The effect of lace-up ankle braces on injury rates in high school basketball players. Am J Sports Med 2011;39(9):1840-1848.
20. McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. Am J Sports Med 2006;34(7):1103-1111.
21. Janssen KW, van Mechelen W, Verhagen EA. Bracing superior to neuromuscular training for the prevention of self reported recurrent ankle sprains: a three-arm randomized controlled trial. Br J Sports Med 2014 January 7. [Epub ahead of print]
22. Petersen W, Rembitzki IV, Koppenburg AG, et al. Treatment of acute ankle ligament injuries: a systematic review. Arch Orthop Trauma Surg 2013;133(8):1129-1141.
23. van den Bekerom MP, Kerkhoffs GM, McCollum GA, et al. Management of acute lateral ankle ligament injury in the athlete. Knee Surg Sports Traumatol Arthrosc 2013;21(6):1390-1395.
24. Olmsted LC, Vela LI, Denegar CR, Hertel J. Prophylactic ankle taping and bracing: a numbers-needed-to-treat and cost-benefit analysis. J Athl Train 2004;39(1):95-100.
25. Verhagen EA, Bay K. Optimising ankle sprain prevention. A critical review and practical appraisal of the literature. Br J Sports Med 2010;44(15):1082-1088.
26. Corzatt RD, Groppel JL, Pfautsch E, Boscardin J. The biomechanics of head-first versus feet-first sliding. Am J Sports Med 1984;12(3):229-232.
27. Kane SM, House HO, Overgaard KA. Head-first versus feet-first sliding: a comparison of speed from base to base. Am J Sports Med 2002;30(6):834-836.
28. Hosey RG, Puffer JC. Baseball and softball sliding injuries. Incidence, and the effect of technique in collegiate baseball and softball players. Am J Sports Med 2000;28(3):360-363.
29. Janda DH, Bir C, Kedroske B. A comparison of standard vs. breakaway bases: an analysis an analysis of a preventative intervention for softball and baseball foot and ankle injuries. Foot Ankle Int 2001;22(10):810-816.
30. Janda DH, Wojtys EM, Hankin FM, Benedict ME. Softball sliding injuries: A prospective study comparing standard and modified bases. JAMA 1988;259(12):1948-1950.
31. Jozsa L, Kvist M, Balint BJ, et al. The role of recreational sports activity in Achilles tendon rupture. A clinical, pathoanatomical and sociological study of 292 cases. Am J Sports Med 1989;17(3):338-343.
32. Leppilahti J, Orava S. Total Achilles tendon rupture: a review. Sports Med 1998;25(2):79-100.
33. Wertz J, Galli M, Borchers JR. Achilles tendon rupture: risk assessment for aerial and ground athletes. Sports Health 2013;5(5):407-409.
34. Kader D, Saxena A, Movin T, Mafulli M. Achilles tendinopathy: some aspects of basic science and clinical management. Br J Sports Med 2002;36(4):239-249.
35. Maffulli N. Current concepts review: rupture of the Achilles tendon. J Bone Joint Surg Am 1999;81:1019-1036 .
36. Yinger K, Mandelbaum BR, Almekinders LC. Achilles rupture in the athlete: current science and treatment. Clin Podiatr Med Surg 2002;19(2):231-250.
37. Hess GW. Achilles tendon rupture: a review of etiology, population, anatomy, risk factors, and injury prevention. Foot Ankle Spec 2010;3(1):29-32.
38. Sugimoto K, Kasanami R, Iwai M, et al. Achilles tendon rupture associated with injury of the calcaneofibular ligament. J Orthop Trauma 2003;17(7):534-535.
39. Miller D, Waterston S, Reaper J, et al. Conservative management, percutaneous or open repair of acute Achilles tendon rupture: a retrospective study. Scott Med J 2005;50(4):160-165.
40. Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med 2012;40(9):2154-2160.
41. Jiang N, Wang B, Chen A, et al. Operative versus nonoperative treatment for acute Achilles tendon rupture: a meta-analysis based on current evidence. Int Orthop 2012;36(4):765-773.
42. Soroceanu A, Sidhwa F, Arabi S, et al. Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials. J Bone Joint Surg Am 2012;94(23):2136-2143.
43. Jackson G, Sinclair VF, McLaughlin C, Barrie J. Outcomes of functional weight-bearing rehabilitation of Achilles tendon ruptures. Orthopedics 2013;36(8):e1053-1059.
44. Cetti R, Christensen SE, Ejsted R, et al. Operative versus nonoperative treatment of Achilles tendon rupture. A prospective randomized study and review of the literature. Am J Sports Med 1993;21(6):791-799.
45. van der Linden-van der Zwaaq HM, Nelissen RG, Sintenie JB. Results of surgical versus non-surgical treatment of Achilles tendon rupture. Int Orthop 2004;28(6):370-373.
46. Parekh SG, Wray WH 3rd, Brimmo O, et al. Epidemiology and outcomes of Achilles tendon ruptures in the National Football League. Foot Ankle Spec 2009;2(6):283-286.
47. Amin NH, Old AB, Tabb LP, et al. Performance outcomes after repair of complete Achilles tendon ruptures in National Basketball Association players. Am J Sports Med 2013;41(8):1864-1868.
48. George E, Harris AH, Dragoo JL, Hunt KJ. Incidence and risk factors for turf toe injuries in intercollegiate football: data from the national collegiate athletic association injury surveillance system. Foot Ankle Int 2014;35(2):108-115.
49. Burge AJ, Gold SL, Potter HG. Imaging of sports-related midfoot and forefoot injuries. Sports Health 2012;4(6):518-534.
50. McCormick JJ, Anderson RB. Turf toe: anatomy, diagnosis and treatment. Sports Health 2010;2(6):487-494.
51. Frimenko RE, Lievers W, Coughlin MJ, et al. Etiology ad biomechanics of first metatarsophalangeal joint sprains (turf toe) in athletes. Crit Rev Biomed Eng 2012;40(1):43-61.
52. Clanton TO, Ford JJ. Turf toe injury. Clin Sports Med 1994;13(4):731-741.
53. Nunley JA, Vertullo CJ. Classification, investigation, and management of midfoot sprains: Lisfranc injuries in the athlete. Am J Sports Med 2002;30(6):871-878.
54. Myerson MS, Cerrato RA. Current management of tarsometatarsal injuries in the athlete. J Bone Joint Surg Am 2008;90(11):2522-2533.
55. Thomas JL, Christensen JC, Kravitz SR, et al. The diagnosis and treatment of heel pain: a clinical practice guideline-revision 2010. J Foot Ankle Surg 2010;49(3 Suppl):S1-19.
56. Kindred J, Trubey C, Simons SM. Foot injuries in runners. Curr Sports Med Rep 2011;10(5):249-254.
57. DeMaio M, Paine R, Mangine RE, Drez D Jr. Plantar fasciitis. Orthopedics 1993;16(10):1153-1163.
58. Daniels CJ, Morrell AP. Chiropractice management of pediatric plantar fasciitis: a case report. J Chiropr Med 2012;11(1):58-63.
59. Karagounis P, Tsironi M, Prionas G, et al. Treatment of plantar fasciitis in recreational athletes: two different therapeutic protocols. Foot Ankle Spec 2011;4(4):226-234.
60. Iwamoto J, Takeda T. Stress fractures in athletes: review of 196 cases. J Orthop Sci 2003;8(3):273-278.
61. Brukner P, Bradhaw C, Khan KM, et al. Stress fractures: a review of 180 cases. Clin J Sport Med 1996;6(2):85-89.
62. Bartz RL, Marymont JV. Tarsal navicular fractures in Major League Baseball players at bat. Foot Ankle Int 2001;22(11):908-910.
63. Smith JS, Flemister AS. Complete cuboid dislocation in a professional baseball player. Am J Sports Med 2006;34(1):21-23.
64. Leri JP. Heel pain in a young adolescent baseball player. J Chiropr Med 2004;3(2):66-68.
65. Walter JH, Ng GK. The evaluation of cleated shoes with the adolescent athlete in soccer. The Foot 2002;12(3):158-165.





