
 Identifying loading patterns associated with Jones fractures and other common sports-related injuries can assist with the development of custom modifications to footwear, insoles, and training programs to help reduce injury rates and enhance athletic careers.
Identifying loading patterns associated with Jones fractures and other common sports-related injuries can assist with the development of custom modifications to footwear, insoles, and training programs to help reduce injury rates and enhance athletic careers.
By Yannick Goeb, Nate Wilcox-Fogel, and Kenneth J. Hunt, MD
Foot and ankle injuries are common in the athletic population, particularly in athletes participating in field and court sports. In fact, an internal review of National Collegiate Athletic Association athletes in Stanford University’s carefully kept injury database indicates that more than one quarter (27%) of injuries in athletes are to the foot, ankle, or both.1 These injuries can often impact performance, result in missed time from participation, and in some cases require surgery or other interventions to return the athlete to their sport.
Much has been published in the scientific literature about “static” mechanical risk factors for foot and ankle injuries.2-4 These are factors such as foot alignment, stiffness, and plantar pressures, which are generally measured on examination or x-rays, with the athlete standing still or taking a single step. Until recently, very little was known about “dynamic” mechanical risk factors for injuries to the foot and ankle during sports activities. These factors must be measured while the athlete is participating in an athletic activity such as running, jumping, or changing direction (ie, cutting).
Identification of dynamic risk factors in athletes can be a challenge since many loading assessment techniques are too cumbersome or inaccurate to give meaningful data. For example, pressure mats are commonly used to measure static pressures or pressures associated with a single step in the middle of a gait or activity protocol. The problem is that it is difficult to know whether this one step—especially if the study participant knows which step will be measured—is representative of the participant’s gait or movement patterns, which can be variable. In addition, while assessment during walking or running is more difficult than a static assessment, it is even more difficult to obtain data on cutting, landing, and other sport-specific activities.
Advances in insole-based plantar pressure measurement technology allow for calibrated and accurate quantification of dynamic loads at specific sites in the foot during athletic activities.5 We are able to apply this technology to the athletic population, in the hope of identifying risk factors for foot injuries and introducing preventive measures to correct or accommodate for excessive mechanical loading.
The best way to identify these risk factors is to prospectively screen a group of athletes and follow them to see which sustain injuries, but that is an expensive and logistically prohibitive undertaking for most researchers. An alternative approach is to assess athletes who have already been successfully treated for the injury.
The Jones fracture
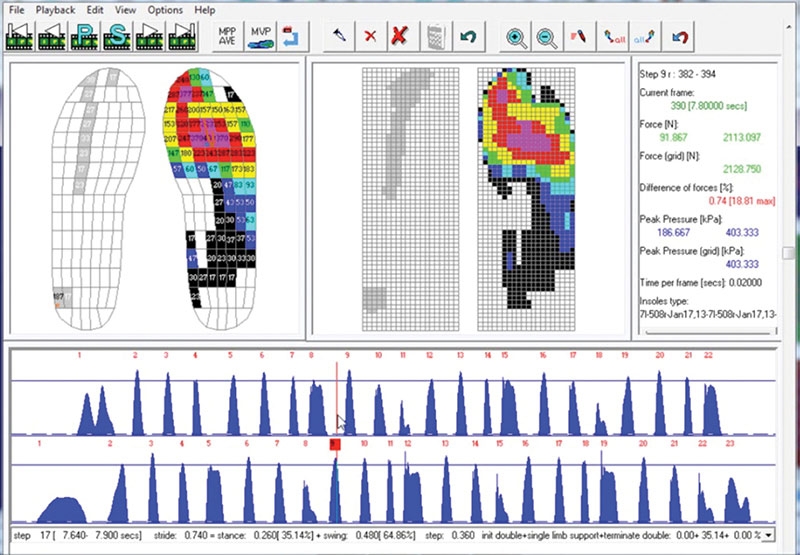
Figure 1. Novel Emed software interface. Steps are shown as pressure peaks in the lower panel (blue peaks). Sensor elements in the insole are represented by colored rectangles in the interface (upper left panel). Image courtesy of Novel.
Fractures of the base of the fifth metatarsal (also called the Jones fracture for Sir Robert Jones, the British orthopedic surgeon who first described the injury)6 are relatively common in field and court athletes. Several high-profile athletes have experienced this injury, and it is not always inconsequential. Jones fractures are broadly accepted to occur because of a buildup of stress at this location in the bone (the fifth metatarsal is on the lateral side of the foot). Forces from the strong peroneus brevis tendon that attaches the fifth metatarsal, along with impact forces during running and cutting, cause the stress buildup.7

It’s well known that one risk factor for Jones fracture is a cavovarus foot with a high arch, in which the heel bone sits slightly inward from its normal position, exposing the fifth metatarsal to higher loads.8 A cavovarus foot alone is unlikely to cause enough stress buildup to cause a Jones fracture in an inactive person but, in athletes, this part of the foot experiences tremendous force. Often the fracture is associated with a seemingly minor impact or inversion injury, the bone having been weakened by many preceding impact forces.
Due to rates of slow healing, nonhealing, and refracture after healing, the majority of Jones fractures in athletes are treated surgically. Surgery involves placing a screw into the fifth metatarsal bone, crossing and compressing the fracture, and stabilizing the bones. Healing rates are high, and recovery generally happens quickly.9
To determine whether athletes with a history of Jones fracture experience increased loads at the fifth metatarsal during athletic activity, thus increasing their risk of stress buildup, we recruited 16 healthy elite athletes (two women) to participate in a study. Half had a history of Jones fracture that had healed uneventfully after surgery, and the other half were controls matched for the same age, sport, and position.
Using a calibrated wireless insole system, we analyzed dynamic loading patterns during sports activities. Each insole has 99 sensors, each sampling at 99 Hz. This provides a lot of information about each step, as illustrated in Figure 1. All athletes performed a series of athletic movements that simulate typical training and competition activities, including walking, running, cutting, and jumping. Previous studies have demonstrated that specific cutting motions such as a crossover pivot may be more relevant for lateral forefoot loading than side cutting.10 Our testing included both side cutting and crossover cutting. We extracted dynamic loading data using the insole software system and compared loading at the fifth metatarsal during each activity between athletes with a history of Jones fracture and controls.
The resulting data showed that athletes with a history of Jones fracture experience significantly higher loads at the base of the fifth metatarsal during athletic activities than control athletes. Interestingly, these differences were evident in walking, running, jumping, and cutting activities, which are among the most common movement patterns in competitive athletes. It’s possible these increased loads during walking and running lead to chronic overloading of the lateral forefoot and contribute to the development of fracture.
Previous studies using other methods of assessing plantar pressure loading have found a decrease in lateral foot loading in athletes with a history of Jones fracture, and no association between cavus foot structure and Jones fracture risk.11 We believe dynamically assessing plantar pressure with insoles, rather than force platforms, provides researchers with more accurate plantar pressure data and may explain the differences seen in our study and previous studies.
We now collect plantar pressure data on all athletes at risk for Jones fractures and other overuse injuries based on their skeletal structure, alignment, and sport. A football lineman with a cavus foot, for example, has a greater risk for Jones fracture than a swimmer.
An important goal in our work characterizing dynamic loading differences in athletes is to identify loading patterns that are modifiable using noninvasive measures such as orthotic devices, mobility and flexibility training, or footwear choice. A study of nonstandardized custom insoles did not demonstrate significant reduction of fifth metatarsal loads in athletes who had suffered a Jones fracture.12 We have now standardized our orthotic technique, and preliminary results of this new method appear to reduce loads.13 Additional study will also help us determine whether identification of at-risk athletes, and subsequent implementation of intervention programs, will reduce injury rates. The results of these and similar studies will help inform understanding of the utility of nonoperative interventions for altering loading patterns of athletes with a particular loading imbalance.
Optimizing injury recovery

Figure 2. Graphic illustrating mean and standard errors for peak pressure (top), contact pressure (center), and impulse (bottom) in three footwear devices in three gait activities. Peak pressure and contact pressure in kPa, impulse in Ns.
A primary goal of rehabilitation following surgical or nonsurgical treatment of any foot injury is reducing mechanical loading in the region of injury. This can be done with crutches or with devices, such as a walking boot, that are designed to reduce loads during walking.
Let’s again look at Jones fractures. After the injury and/or surgery, we want to reduce loads on the lateral aspect of the foot to help ensure complete healing before the athlete returns to sports. Excess force after surgery can slow or even prevent healing.14 However, we want to avoid complete immobilization, as in a cast or nonremovable splint, since this can lead to muscle atrophy and deconditioning.15
Using dynamic load-sensing insoles, we recently compared available offloading rehabilitation devices to see which would best accomplish our objective.16 We recruited 20 active healthy young people with no recent history of foot injury. We had each study participant wear each of three commonly used rehabilitation devices—a CAM (controlled ankle movement) walker boot, a rigid postoperative sandal, and a standard athletic shoe. During heel walking, subjects walked on their heels at 1 m/s and were instructed to keep pressure off the hallux and forefoot.
Our aim was to determine which device most successfully offloaded the fifth metatarsal base during walking, heel walking, and pivoting, all common daily activities. Our results (Figure 2) show the CAM walker boot was associated with significantly lower loads at the fifth metatarsal base in several testing conditions relative to the sandal and shoe.
The CAM walker boot shower reduced contact pressure at the fifth metatarsal during walking and heel walking relative to the postoperative sandal, and during heel walking relative to the shoe. In other testing conditions, there was a trend toward reduced contact pressures in the CAM boot relative to the shoe, though these trends were not statistically significant. There was little observed difference in fifth metatarsal loads between the athletic shoe and the postoperative sandal for any of the conditions tested. This suggests a CAM walker boot is likely a better choice for rehabilitation of Jones fractures than a sandal or shoe.
There are, of course, many factors in addition to load reduction to consider when choosing rehabilitation footwear. Mobility and comfort, for example, may affect practitioners’ and patients’ decisions about footwear devices for the rehabilitative period.
Clinical applications
The observation that increased fifth metatarsal loads during repetitive athletic activities such as walking and running correlate with an athlete’s history of fifth metatarsal stress fracture highlights the role that repetitive loading patterns may play during long periods of competition or training.
Wireless insole-based plantar pressure measurement systems allow an accurate and reproducible assessment of loading patterns and an effective means of understanding an athlete’s loading mechanics, as well as the effectiveness of interventions. As sensor technology continues to advance, basic pressure insole systems will likely become more available for a greater number of practitioners and will undoubtedly become a more common tool for risk factor assessment.
We foresee a future in which patients are risk-stratified based on their plantar pressure distributions as compared with a large group of healthy age-matched controls. Developing a large database of patients to better understand the “normal” plantar pressure distributions in different foot structures will require ongoing testing.
Topological data analysis

Figure 3. Sample topological network created with 60-plus elite athletes, each represented by a node and spatially organized based on loading patterns during common athletic activities. Nodes highlighted represent athletes with a history of Jones fracture.
The use of wireless plantar pressure insoles allows for quantification of loading patterns in elite athletes during a variety of athletic activities. The amount of data generated by even a single trial of data sampling is substantial. Our team has used innovative data analysis methods to better handle our large data sets. One such method is called “topological data analysis,” or TDA, which allows for visualization of complex data sets in a spatial network of nodes organized by statistical similarity. This method has been used in oncology to study genetic similarities between tumor samples, as well as in sports analytics to better understand athletes’ performance.17
In our use of TDA, each athlete is represented as a node in a topological network. The similarities are assessed based on each athlete’s plantar pressure data, whereby athletes with similar measurements across all chosen dimensions are more closely connected to each other. We then use a software program to determine which athletes are most and least similar to each other based on clustering of specific data points in the statistical network. A sample of a TDA network from our data, highlighting athletes with a history of Jones fracture, is shown in Figure 3.
Through this athlete risk segmentation, we can identify “types” of athletes who are more or less at risk for certain injuries based on their plantar pressure data. We can also determine associations between certain loading patterns and different sports, positions, and genders, creating relationships between an athlete’s dynamic loading profile and his or her injury history or risk. At this stage, we are using this method of risk stratification in a research setting only. In the future, we hope to better understand foot and ankle injury risk using TDA networks and implement topological data analysis into clinical practice.
Summary
The end goal of this collaborative work is prevention of injuries in athletes by systematically identifying risk factors for injury and instituting preventive measures. Our work thus far has allowed us to identify a pattern of increased loads at the fifth metatarsal in athletes with a history of Jones fracture and to compare the degree of offloading provided by different rehabilitative footwear options.
Additional analyses are underway with our data system to identify loading patterns associated with other common injuries. Ultimately, custom modifications to footwear, insoles, and training programs may help reduce injury rates and enhance athletic careers.
Yannick Goeb is a fourth- year medical student and Nate Wilcox-Fogel is a third-year medical student at the Stanford University School of Medicine in California. Kenneth J. Hunt, MD, is an associate professor and chief of Foot and Ankle Surgery at the University of Colorado School of Medicine in Aurora.
- Hunt KJ. Unpublished 2014 data. Stanford University Department of Orthopaedic Surgery.
- Adirim TA, Cheng TL. Overview of injuries in the young athlete. Sports Med 2003;33(1):75-81.
- O’Loughlin PF, Murawski CD, Egan C, Kennedy JG. Ankle instability in sports. Phys Sportsmed 2009;37(2):93-103.
- Shindle MK, Endo Y, Warren RF, et al. Stress fractures about the tibia, foot, and ankle. J Am Acad Orthop Surg 2012;20(3):167-176.
- Orlin MN, McPoil TG. Plantar pressure assessment. Phys Ther 2000;80(4):399-409.
- Nunley JA. Fractures of the base of the fifth metatarsal: the Jones fracture. Orthop Clin North Am 2001;32(1):171-180.
- Lawrence SJ, Botte MJ. Jones’ fractures and related fractures of the proximal fifth metatarsal. Foot Ankle 1993;14(6):358-365.
- Raikin SM, Slenker N, Ratigan B. The association of a varus hindfoot and fracture of the fifth metatarsal metaphyseal-diaphyseal junction: the Jones fracture. Am J Sports Med 2008;36(7):1367-1372.
- Porter DA, Duncan M, Meyer SJ. Fifth metatarsal Jones fracture fixation with a 4.5-mm cannulated stainless steel screw in the competitive and recreational athlete: a clinical and radiographic evaluation. Am J Sports Med 2005;33(5):726-733.
- Queen RM, Haynes BB, Hardaker WM, Garrett WE Jr. Forefoot loading during 3 athletic tasks. Am J Sports Med 2007;35(4):630-636.
- Hetsroni I, Nyska M, Ben-Sira D, et al. Analysis of foot structure in athletes sustaining proximal fifth metatarsal stress fracture. Foot Ankle Int 2010;31(3):203-211.
- Hunt KJ, Goeb Y, eds. Dynamic load assessment at the 5th metatarsal base in elite athletes. Presented at the ESSKA Congress, Amsterdam, Netherlands, May 2014.
- Goeb Y, Hunt KJ. Unpublished data.
- Konkel KF, Menger AG, Retzlaff SA. Nonoperative treatment of fifth metatarsal fractures in an orthopaedic suburban private multispeciality practice. Foot Ankle Int 2005;26(9):704-707.
- Rosenberg GA, Sferra JJ. Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8(5):332-338.
- Hunt KJ, Goeb Y, Esparza R, et al. Site-specific loading at the fifth metatarsal base in rehabilitative devices: implications for Jones fracture treatment. PM R 2014;6(11):1022-1029.
- Lum PY, Singh G, Lehman A, et al. Extracting insights from the shape of complex data using topology. Sci Reports 2013;3:1236.





