
 By Karl F. Orishimo, MS, CSCS, and Takumi Fukunaga, DPT, ATC, CSCS
By Karl F. Orishimo, MS, CSCS, and Takumi Fukunaga, DPT, ATC, CSCS
The effectiveness of eccentric training for the prevention and rehabilitation of hamstring strains has been established in the medical literature. The next step is to identify an eccentric hamstring exercise that addresses the limitations of existing eccentric strengthening techniques.
Hamstring muscle strain is a very common injury in many sports such as soccer, rugby, and track and field.1-4 Recurrence rates for this injury have been reported to be as high as 30%.5 The significant time loss to the athlete associated with this injury, combined with the high rate of reinjury, has spurred much research into rehabilitation and prevention methods. Eccentric exercises have emerged as essential components of effective rehabilitation6,7 and injury prevention programs.8
Injury mechanism
Before examining the utility of eccentric exercises for treating and preventing hamstring strains, an understanding of a common injury mechanism is necessary. Hamstring strains typically occur during high-speed running and cutting. Motion analysis studies of sprinting have shown that peak hamstring lengthening occurs during the late swing phase.9,10 During this phase, the hamstrings are acting eccentrically to slow the lower leg and to prepare and position the leg for ground contact. Schache et al11 were fortunate to record a hamstring strain injury during a sprinting trial and confirmed that the injury most likely occurs around this point in the gait cycle. With the understanding that the hamstrings must be conditioned to withstand the high forces associated with this point in the gait cycle, the authors recommended that “hamstring injury prevention and rehabilitation programs should preferentially target strengthening exercises that involve eccentric contractions performed with high loads at longer musculotendon lengths.”12
Rehabilitation after hamstring strain
Given the high rate of reinjury, it is essential for an athlete who sustains a primary hamstring strain to undergo a formal rehabilitation program before returning to his or her preinjury level of sports. At our institution, we utilize a three-phase, evidence-based rehabilitation program and a battery of tests before clearing an athlete for full sports participation. This program is rooted in the basic science of muscle injury and treatment methods validated in previous clinical studies. A comprehensive description of our rehabilitation program was published recently by Schmitt et al.13
![Figure 1: The Nordic hamstring exercise. (Reprinted with permission from Arnason A, Andersen TE, Holme I, et al. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports 2008;18[1]:40-48.)23](https://lermagazine.com/wp-content/uploads/2015/02/2hamstring-figure1-copy.jpg)
Figure 1: The Nordic hamstring exercise. (Reprinted with permission from Arnason A, Andersen TE, Holme I, et al. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports 2008;18[1]:40-48.)23
The athlete may present with significant pain, discoloration, and gait deviations. Use of therapeutic modalities (eg, ice, electric stimulation, pulsed therapeutic ultrasound) and manual soft tissue mobilization may be started immediately after the injury and can be effective for pain modulation. If a significant gait deviation is observed, then use of crutches for ambulation is recommended. Experimental evidence suggests that active mobilization after muscle injury results in superior histochemical and biomechanical recovery compared to immobilization,14 and riding on a stationary bike is effective for encouraging early active motion.
Further, isometric hamstring contractions are performed at multiple knee flexion angles (eg, 30°, 60°, 90°) to start exerting tension in the injured muscle. Progressive introduction of tension in the injured muscle is believed to strengthen the scar between fractured muscle fibers and help approximate the fiber stumps.15 It is important at this phase of rehabilitation that all activities and rehabilitation exercises are performed without pain.
Once the athlete is able to walk with a normal gait pattern and perform a submaximal (up to 75%) isometric contraction of the hamstrings without pain, the athlete is progressed to phase 2 of the rehabilitation. The objectives of this second phase are to increase isotonic hamstring strength throughout the range of motion and to improve neuromuscular control of the lower extremity in preparation for sport-specific movements. Appropriate exercises in this phase include isotonic hamstring curls, deadlifts, single-leg deadlifts, Nordic hamstring exercises,6,13 as well as other eccentric-biased exercises, such as the L-protocol exercises described by Askling et al.16 Upon achieving full motion and minimal strength deficit (< 20% of contralateral side) in the hamstrings, the athlete is progressed to phase 3.

The third phase of rehabilitation involves sport-specific drills and lengthened-state eccentric exercises. The sport-specific drills may consist of sprints, agility drills, and plyometric training. The eccentric-biased exercises are progressed to performing them in positions where the hamstrings are under maximal tension. This lengthened-state method of eccentric training is thought to strengthen the hamstrings in their longer muscle length and contribute to reduction in incidence of recurrent hamstring strains.13
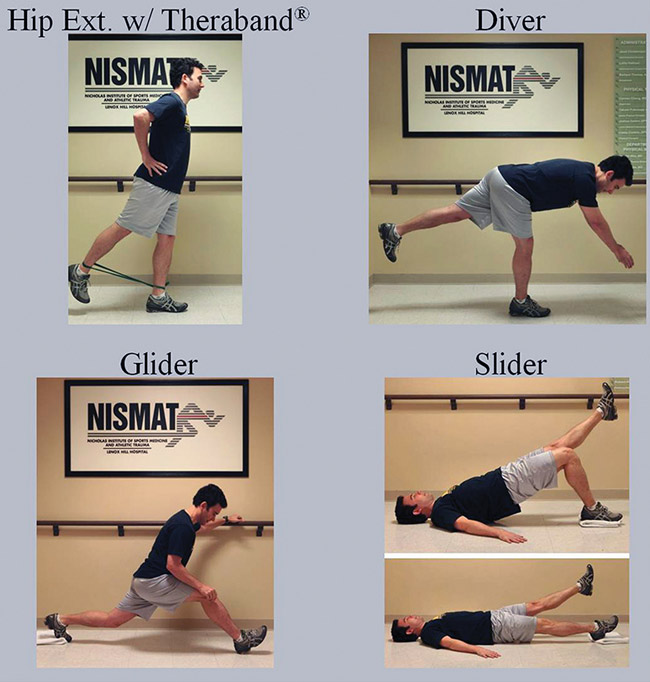
Figure 2: Four eccentrically biased exercises studied by Orishimo and McHugh. The hip extension, Diver, and Slider exercises were adapted from Askling et al.16 For the Glider, subjects performed a supine single-leg bridge and then lowered their torso to the floor by extending the knee of the supporting leg and sliding the foot forward. A rep was completed when the subject lowered his or her body to the floor and then returned to the starting position by sliding both feet into full knee flexion, then assuming the bridge position and lifting one leg off the floor.
Once the athlete has completed all three phases of the rehabilitation program without pain or compensatory patterns, a battery of tests are carried out to ensure the athlete can safely return to full sport participation. Strength testing of the hamstrings is performed with an isokinetic or hand-held dynamometer and compared with the noninjured side. A manual muscle test may be performed in the prone or supine position if a dynamometer is not available. The athlete must have minimal strength deficit (less than a 10% deficit relative to the contralateral side, as measured with a dynamometer) throughout the range of motion before returning to sports participation. Recently, a rigorous functional test, named the H-test, has been proposed as a tool to determine safety in returning to sports after hamstring injury.17 Using this H-test as the primary return-to-sport criterion, Askling et al16 reported only one case of hamstring reinjury among 75 athletes followed over 12 months after return to sports.
Once an athlete has been cleared to return to sport participation, we recommend incorporating the eccentric exercises (eg, Nordic hamstring exercise, L-protocol, etc) into his or her strength and conditioning routine, as these exercises have been shown to reduce recurrence of hamstring strains.1,16
Why eccentrics?
Eccentric exercises have been shown to add sarcomeres in series18 and increase muscle strength at longer lengths (ie, the descending limb of the length-tension curve).19 These physiological adaptations act to protect a muscle against injury by reducing the damage caused by repeated eccentric contractions. Studies by Kilgallon et al20 and Mjolsnes et al21 have compared the effects of eccentric versus concentric hamstring strengthening exercises and showed that increases in strength at longer muscle lengths occur only after bouts of eccentric exercises. Therefore, training the hamstrings eccentrically may give them the ability to resist the high forces experienced during high-speed running and to avoid disruption of the muscle fibers.
Nordic hamstring exercise
A popular and highly effective eccentric exercise for the prevention of hamstring strains is the Nordic hamstring exercise (NHE). To perform this exercise, the athlete starts in an upright kneeling position with arms at the sides and a partner holding the ankles on the ground. From this position, the athlete falls forward and, as slowly as possible, lowers the torso to the ground using only the hamstrings. In the end position, the athlete is lying prone on the ground with straight knees, hips, and torso (Figure 1). The athlete then returns to the starting position by pushing up with the hands while using minimal concentric contractions of the hamstrings.
Brockett et al22 demonstrated that a single bout of the NHE (12 sets of six repetitions) produced a shift in the angle of peak torque toward longer muscle lengths. Additionally, this adaptation was shown to have a long-lasting protective effect against subsequent muscle damage. Studies in soccer players have shown an 11% increase in eccentric hamstring strength21 and a 65% reduction in hamstring strains in teams that used the NHE compared with those that did not.23 Additionally, in a randomized controlled trial, Petersen et al24 found that using the NHE was associated with a rate of recurrent hamstring injury that was 85% lower than the recurrence rate in the control group, which followed their usual training program.
Although the NHE has been shown to be very effective in preventing hamstring strains, it does have a few limitations. First, a partner is needed to hold the ankles while the athlete performs the exercise. While this may work well in a team setting, it may not be suitable in a rehabilitation or home exercise program. Secondly, the NHE is a bilateral exercise (ie, performed on both legs simultaneously). This could allow for one side to compensate for the other and to further reinforce side-to-side strength imbalances in patients rehabilitating a hamstring strain. These limitations have led researchers to investigate alternative eccentric exercises that are just as effective in preventing injury.
Other eccentric exercises
In a prospective randomized controlled clinical trial, Askling et al16 compared the time to return to sport in soccer players treated for hamstring strains using the eccentric “L-protocol” compared with conventional rehabilitation exercises consisting of stretching and concentric strengthening. All three exercises in the L-protocol (the Extender, the Diver, and the Glider) were simple unilateral eccentric exercises that participants performed using minimal equipment and the weight of their body as resistance. The time required to return to sport following the hamstring injury was 45% shorter in players performing the eccentric protocol than those performing the conventional protocol. Additionally, there were no reinjuries during the one-year follow-up period in the eccentric training group, compared with two in the conventional exercise group. The same authors found similar results in sprinters and jumpers using the L-protocol compared with conventional strengthening and stretching.25
To further understand the underlying causes of these clinical results, Orishimo and McHugh26 investigated the effects of an eccentrically biased exercise program inspired by the L-protocol on the angle-torque relationship of the knee flexors in 12 healthy individuals. A secondary objective was to characterize the electromyographic activity of the hamstrings during each of the four exercises (Figure 2). After a four-week training period, overall knee flexor strength increased by about 10%, but the strength gains were not angle-specific (ie, there was no shift toward longer muscle lengths). Although these exercises were considered eccentrically biased, electromyographic data showed substantial hamstring activity during the concentric portions of the exercises, as well. Unlike the Nordic hamstring exercise, which is exclusively eccentric, the L-protocol exercises require considerable concentric contraction to return to the starting position. Therefore, considering the findings of Kilgallon et al20 that the angle of peak isometric torque increased with concentric training but decreased with eccentric training, it is possible that the concentric portions of these exercises may be counteracting the adaptations produced by the eccentric portions.
Despite not shifting the angle of peak torque of the hamstrings toward a longer muscle length, these alternative eccentric exercises improved strength, flexibility, and core control, all of which have been shown to be instrumental in reducing the incidence of primary and secondary hamstring strains.27,28 Strength exercises that combine elements of balance and flexibility may accelerate an athlete’s progression through rehabilitation to the return-to-sport phase more effectively than using exercises that address each element individually.
![Figure 3: Lengthened state eccen- tric hamstring strengthening on an isokinetic dynamometer. (Reprinted with permission from Schmitt B, Tyler T, McHugh M. Hamstring in- jury rehabilitation and prevention of reinjury using lengthened state ec- centric training: a new concept. Int J Sports Phys Ther 2012;7[3]:333- 341.)13](https://lermagazine.com/wp-content/uploads/2015/02/2hamstring_Figure-3-copy.jpg)
Figure 3: Lengthened state eccentric hamstring strengthening on an isokinetic dynamometer. (Reprinted with permission from Schmitt B, Tyler T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. Int J Sports Phys Ther 2012;7[3]:333- 341.)13
“Lengthened state” eccentric training
Recently, Schmitt et al13 have introduced and advocated the use of “lengthened state” eccentric exercise to improve hamstring strength at the end of the range of motion. The lengthened state is achieved by combining maximal or near-maximal hip flexion and knee extension, so that the knee flexors are stretched over both the hip and knee articulations (Figure 3). Preliminary data have shown that patients treated with this modified form of eccentric training in the context of a three-phase rehabilitation program had greater hamstring strength at longer muscle lengths and experienced fewer reinjuries than athletes who were noncompliant.29 This type of training, however, requires the use of an isokinetic dynamometer to provide sufficient overload to the muscle, a device that may not be readily available in most physical therapy clinics. Therefore, more research is needed to design eccentric exercises that position the hamstrings in a lengthened state and require little or no equipment.
Conclusions
Eccentric exercises have been shown to be effective in reducing primary and secondary hamstring strains. The NHE is the method used most commonly for injury prevention, but simpler unilateral exercises have also been shown to be highly effective. Lengthened state eccentrics offer targeted training to address weakness at the end of the range of motion. However, the requirement of specialized equipment (an isokinetic dynamometer) to perform this type of training may preclude its use. Future research needs to focus on designing an exercise that produces similar adaptations as the NHE or lengthened state eccentrics, but does not require a partner and can be done with minimal equipment.
Karl F. Orishimo, MS, CSCS, is a biomechanist and research associate at the Nicholas Institute of Sports Medicine and Athletic Trauma at Lenox Hill Hospital in New York City. Takumi Fukunaga, DPT, ATC, CSCS, is a senior physical therapist and research assistant at the Nicholas Institute of Sports Medicine and Athletic Trauma.
- Brooks JH, Fuller CW, Kemp SPT, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med 2006;34(8):1297-1306.
- Elliott MC, Zarins B, Powell JW, Kenyon CD. Hamstring muscle strains in professional football players: a 10-year review. Am J Sports Med 2011;39(4):843-850.
- Woods C, Hawkins RD, Maltby S, et al. The Football Association Medical Research Programme: an audit of injuries in professional football—analysis of hamstring injuries. Br J Sports Med 2004;38(1):36-41.
- Malliaropoulos N, Isinkaye T, Tsitas K, Maffulli N. Reinjury after acute posterior thigh muscle injuries in elite track and field athletes. Am J Sports Med 2011;39(2):304-310.
- Orchard J, Best TM. The management of muscle strain injuries: an early return versus the risk of recurrence. Clin J Sport Med 2002;12(1):3-5.
- Heiderscheit BC, Sherry MA, Silder A, et al. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. J Orthop Sports Phys Ther 2010;40(2):67-81.
- Lorenz D, Reiman M. The role and implementation of eccentric training in athletic rehabilitation: tendinopathy, hamstring strains, and ACL reconstruction. Int J Sports Phys Ther 2011;6(1):27-44.
- Thorborg K. Why hamstring eccentrics are hamstring essentials. Br J Sports Med 2012;46(7):463-465.
- Yu B, Queen RM, Abbey AN, et al. Hamstring muscle kinematics and activation during overground sprinting. J Biomech 2008;41(15):3121-3126.
- Chumanov ES, Schache AG, Heiderscheit BC, Thelen DG. Hamstrings are most susceptible to injury during the late swing phase of sprinting. Br J Sports Med 2012;46(2):90.
- Schache AG, Kim HJ, Morgan DL, Pandy MG. Hamstring muscle forces prior to and immediately following an acute sprinting-related muscle strain injury. Gait Posture 2010;32(1):136-140.
- Schache AG, Dorn TW, Blanch PD, et al. Mechanics of the human hamstring muscles during sprinting. Med Sci Sports Exerc 2012;44(4):647-658.
- Schmitt B, Tyler T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. Int J Sports Phys Ther 2012;7(3):333-341.
- Lehto M, Duance VC, Restall D. Collagen and fibronectin in a healing skeletal muscle injury. An immunohistological study of the effects of physical activity on the repair of injured gastrocnemius muscle in the rat. J Bone Joint Surg Br. 1985;67(5):820-828.
- Järvinen TA, Järvinen TL, Kääriäinen M, et al. Muscle injuries: biology and treatment. Am J Sports Med 2005;33(5):745-764.
- Askling CM, Tengvar M, Thorstensson A. Acute hamstring injuries in Swedish elite football: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br J Sports Med 2013;47(15):953-959.
- Askling CM, Nilsson J, Thorstensson A. A new hamstring test to complement the common clinical examination before return to sport after injury. Knee Surg Sports Traumatol Arthrosc 2010;18(12):1798-1803.
- Lynn R, Talbot JA, Morgan DL. Differences in rat skeletal muscles after incline and decline running. J Appl Physiol 1998;85(1):98-104.
- McHugh MP, Tetro DT. Changes in the relationship between joint angle and torque production associated with the repeated bout effect. J Sports Sci 2003;21(11):927-932.
- Kilgallon M, Donnelly AE, Shafat A. Progressive resistance training temporarily alters hamstring torque-angle relationship. Scand J Med Sci Sports 2007;17(1):18-24.
- Mjølsnes R, Arnason A, Østhagen T, et al. A 10-week randomized trial comparing eccentric vs. concentric hamstring strength training in well-trained soccer players. Scand J Med Sci Sports 2004;14(5):311-317.
- Brockett CL, Morgan DL, Proske U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med Sci Sports Exerc 2001;33(5):783-790.
- Arnason A, Andersen TE, Holme I, et al. Prevention of hamstring strains in elite soccer: an intervention study. Scand J Med Sci Sports 2008;18(1):40-48.
- Petersen J, Thorborg K, Nielsen MB, et al. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med 2011;39(11):2296-2303.
- Askling CM, Tengvar M, Tarassova O, Thorstensson A. Acute hamstring injuries in Swedish elite sprinters and jumpers: a prospective randomised controlled clinical trial comparing two rehabilitation protocols. Br J Sports Med 2014;48(7):532-539.
- Orishimo KF, McHugh MP. The effect of an eccentrically-biased hamstring strengthening home program on knee flexor strength and the length-tension relationship. J Strength Cond Res 2014 Sep 15. [Epub ahead of print]
- Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports 2003;13(4):244-250.
- Sherry MA, Best TM. A comparison of 2 rehabilitation programs in the treatment of acute hamstring strains. J Orthop Sports Phys Ther 2004;34(3):116-125.
- Tyler TF, Schmitt B, Gellert JM, McHugh MP. Eccentric strengthening at long muscle lengths reduces hamstring strain recurrences: results of long term follow-up. Presented at American Orthopaedic Society for Sports Medicine Annual Meeting, Seattle, WA, July 2014.






I enjoyed reading your article.
At Engineered Sports, we’ve published a guide on how to prevent hamstring injuries: https://engineered2win.com/prevent-hamstring-injuries/